Dr Mario Castro discussing GOLD COPD guidelines for allergists. Most patients don’t come in thinking they have COPD, many present to the allergist with cough and “asthma”.
Biomass combustion is the number 1 worldwide cause of COPD, tobacco smoke exposure higher in the US.
Don’t forget about lung cancer screening and alpha-1-AT screening in patients with COPD.
Blood eosinophil level may predict exacerbation rates in COPD.
GOLD 2018 algorithm for COPD:
1. Staging of COPD
2. Symptom assessment - CAT and mMRC
3. Assess risk for exacerbations based on prior hx.
Only smoking cessation has been shown to reduce mortality in COPD - ask, advise, assess, assist, arrange.
Nonpharmacological therapy to manage COPD- smoking cessation, patient education, vaccination, pulmonary rehab, oxygen therapy, and surgical/no surgical alternatives.
ALL COPD patients should be screened for alpha-1 AT deficiency. Don't forget to screen for cancer. Only smoking cessation has been shown to reduce mortality. NRT, vaccination (PPSV-23, PCV-13 and flu) and pulmonary rehab are also of utmost importance.
Dr Hanania, pulmonologist from Baylor, discussed ACO (Asthma-COPD overlap) guidelines. Don’t use term ACOS since the overlap is not a single disease entity.
Up to 65% of COPD patients show significant reversibility on spirometry.
ACO patients should be treated with ICS as first-line therapy, then think about LABA, LAMA, LABA/LAMA.
Dr Azar discussed humoral immunodeficiency in COPD pts with severe exacerbations.
“IgG subclasses don’t have a role in diagnosing primary immunodeficiency if total IgG is normal” - Dr Antoine Azar.
Consider antibody deficitency in patients with frequent COPD exacerbations.
This is a Twitter summary from #ACAAI18 meeting based on tweets by the following allergists: @mrathkopf @asthmallergydoc @kparksmd
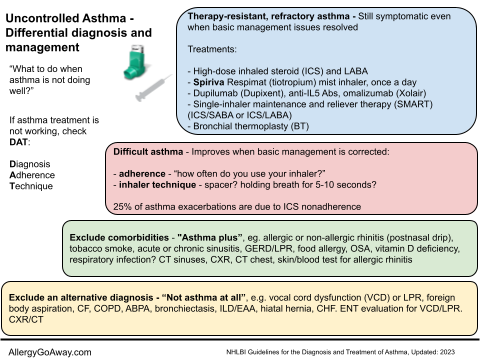
Uncontrolled asthma: “What to do when asthma is not doing well?” (click to enlarge the image).
Biomass combustion is the number 1 worldwide cause of COPD, tobacco smoke exposure higher in the US.
Don’t forget about lung cancer screening and alpha-1-AT screening in patients with COPD.
Blood eosinophil level may predict exacerbation rates in COPD.
GOLD 2018 algorithm for COPD:
1. Staging of COPD
2. Symptom assessment - CAT and mMRC
3. Assess risk for exacerbations based on prior hx.
Only smoking cessation has been shown to reduce mortality in COPD - ask, advise, assess, assist, arrange.
Nonpharmacological therapy to manage COPD- smoking cessation, patient education, vaccination, pulmonary rehab, oxygen therapy, and surgical/no surgical alternatives.
ALL COPD patients should be screened for alpha-1 AT deficiency. Don't forget to screen for cancer. Only smoking cessation has been shown to reduce mortality. NRT, vaccination (PPSV-23, PCV-13 and flu) and pulmonary rehab are also of utmost importance.
Dr Hanania, pulmonologist from Baylor, discussed ACO (Asthma-COPD overlap) guidelines. Don’t use term ACOS since the overlap is not a single disease entity.
Up to 65% of COPD patients show significant reversibility on spirometry.
ACO patients should be treated with ICS as first-line therapy, then think about LABA, LAMA, LABA/LAMA.
Dr Azar discussed humoral immunodeficiency in COPD pts with severe exacerbations.
“IgG subclasses don’t have a role in diagnosing primary immunodeficiency if total IgG is normal” - Dr Antoine Azar.
Consider antibody deficitency in patients with frequent COPD exacerbations.
This is a Twitter summary from #ACAAI18 meeting based on tweets by the following allergists: @mrathkopf @asthmallergydoc @kparksmd
Uncontrolled asthma: “What to do when asthma is not doing well?” (click to enlarge the image).