Another reversal from #ACAAI18: Asthma is not a significant predictor for severe food allergy.
Most tree nut individuals may only be allergic to 1 — 2 tree nuts, but not to 5–6.
Alway try to offer oral challenge in walnut positive skin tested patients due to sensitization.
@asthmaallergydoc: All pecan allergic patients are allergic to walnut! All pistachio allergic patients are allergic to cashews. The opposite is not always true (66% for both). Oral food challenges remain gold standard for diagnosis.
Food allergy: uncertain evidence regarding role of diet during pregnancy/infancy and subsequent allergy.
Brian Schroer MD @Brian34Schroer: Hold epi like a microphone. With blue to sky orange to the thigh.
Risk assessment criteria for oral food challenges: https://twitter.com/AllergyKidsDoc/status/1063835973908189187
Peanut OIT
Dr. David Fleischer: Peanut OIT likely coming in 2019, however, are practices prepared for the increase in phone calls, treatment of reactions, policies and procedures and education of staff to provide this service?
Providers should present options for oral immunotherapy in a unbiased fashion and tailor the chosen therapy (or continued avoidance) based on the patient/caregiver preferences.
Many allergists still refer to Dr. Sampson's 95% PPV IgE cutoffs based on his work at Johns Hopkins https://www.ncbi.nlm.nih.gov/pubmed/15842229
However, the IgE levels don't apply to unexposed pts, doesn't tell us the severity of the reaction, and 30% of patients would be predicted to have a positive challenge at the "negative" 0.35 kU/L food specific IgE.
Food allergy history critical elements: what did they eat, what form was it? Had they eaten it before? How much? Have they eaten it again (even other forms)? Was it a protein vs. dye?
Estimating pretest probability of disease based on history: https://www.jaci-inpractice.org/article/S2213-2198(12)00019-0/fulltext
Controversial tests in food allergy
Dr. John Kelso presented on controversial tests in food allergy.
ALCAT test: change in volume of WBC (change and distribution of cell size) as determined by flow cytometry after incubation with foods, there are no published studies in peer reviewed journals regarding the predictive value of the ALCAT test for food allergy.
Kelso article describing unproven diagnostic tests for food allergy: https://www.jaci-inpractice.org/article/S2213-2198(17)30704-3/abstract
IgG/IgG4 food allergy testing - claims to predict food "sensitivities" such as irritable bowel syndrome. IgG food allergy testing studies are retrospective in nature and may be subject to bias.
This is a Twitter summary from #ACAAI18 meeting based on tweets by the following allergists:
@DrGerryLee @WAOJM @alexeigonzmd
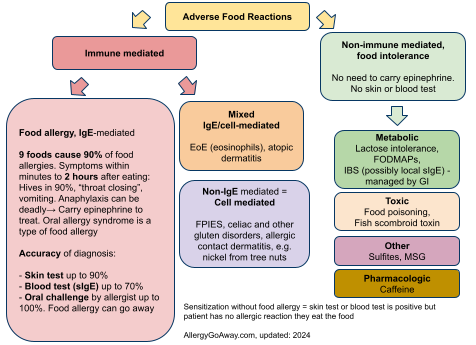
Adverse Food Reactions (click to enlarge the image).
Most tree nut individuals may only be allergic to 1 — 2 tree nuts, but not to 5–6.
Alway try to offer oral challenge in walnut positive skin tested patients due to sensitization.
@asthmaallergydoc: All pecan allergic patients are allergic to walnut! All pistachio allergic patients are allergic to cashews. The opposite is not always true (66% for both). Oral food challenges remain gold standard for diagnosis.
Food allergy: uncertain evidence regarding role of diet during pregnancy/infancy and subsequent allergy.
Brian Schroer MD @Brian34Schroer: Hold epi like a microphone. With blue to sky orange to the thigh.
Risk assessment criteria for oral food challenges: https://twitter.com/AllergyKidsDoc/status/1063835973908189187
Peanut OIT
Dr. David Fleischer: Peanut OIT likely coming in 2019, however, are practices prepared for the increase in phone calls, treatment of reactions, policies and procedures and education of staff to provide this service?
Providers should present options for oral immunotherapy in a unbiased fashion and tailor the chosen therapy (or continued avoidance) based on the patient/caregiver preferences.
Many allergists still refer to Dr. Sampson's 95% PPV IgE cutoffs based on his work at Johns Hopkins https://www.ncbi.nlm.nih.gov/pubmed/15842229
However, the IgE levels don't apply to unexposed pts, doesn't tell us the severity of the reaction, and 30% of patients would be predicted to have a positive challenge at the "negative" 0.35 kU/L food specific IgE.
Food allergy history critical elements: what did they eat, what form was it? Had they eaten it before? How much? Have they eaten it again (even other forms)? Was it a protein vs. dye?
Estimating pretest probability of disease based on history: https://www.jaci-inpractice.org/article/S2213-2198(12)00019-0/fulltext
Controversial tests in food allergy
Dr. John Kelso presented on controversial tests in food allergy.
ALCAT test: change in volume of WBC (change and distribution of cell size) as determined by flow cytometry after incubation with foods, there are no published studies in peer reviewed journals regarding the predictive value of the ALCAT test for food allergy.
Kelso article describing unproven diagnostic tests for food allergy: https://www.jaci-inpractice.org/article/S2213-2198(17)30704-3/abstract
IgG/IgG4 food allergy testing - claims to predict food "sensitivities" such as irritable bowel syndrome. IgG food allergy testing studies are retrospective in nature and may be subject to bias.
This is a Twitter summary from #ACAAI18 meeting based on tweets by the following allergists:
@DrGerryLee @WAOJM @alexeigonzmd
Adverse Food Reactions (click to enlarge the image).