Michael Schatz discussed Asthma and Drug Allergy in this year's JACI-In Practice.
92% of patients with difficult to control asthma had at least one medical comorbidity. What were those comorbidities? Obesity, anxiety/depression, GERD, cardiovascular disease. Asthma: 90% of pts with severe asthma have at least one comorbidity, 70% have more than 2. Many co-morbidities are bi-directional, ie if you treat one, you get improvement in the other and vice versa.
Non pharma management of asthma: exercise - high intensity, diet - high protein/low glycemic diet - you need both to improve asthma control.
Step down RX for asthma who are well controlled for 3 months: stopping LABA was associated with greater decline in lung function and more hospitalizations, maybe we need longer than 3 months of control.
Pts who cough and failed ICS/LABA combo inhaler improved with Spiriva. Likely through modulating cough reflex sensitivity, despite no difference in FEV1.
Only 22% of large group of health care providers used asthma inhalers correctly (JACI-IP 2018;6:987). Most common specific errors of healthcare professionals with not using their inhalers correctly: https://twitter.com/MatthewBowdish/status/1087905408486825984
Check our JACI-IP 2018;6:1246 for interesting article on skin testing for suspected iodinated contrast media hypersensitivity.
For contrast reactions: consider SPT :prick undiluted, ID 1:10 dilution - not irritating. Pretreatment for contrast reactions does not appear to be helpful. Approach to RCM reactions: https://twitter.com/RayFirszt/status/1087908037426204674
Controversies in beta-lactam allergy covered in JACI-IP:
1. Role of skin testing vs direct challenge
2. Length of challenge (single dose vs multiple day)
3. Cephalosporin cross-reactivity with PCN and other cephalosporins
Optimal length of penicillin challenge is unclear. 5 days seems reasonable to rule out delayed non severe reactions.
Current Kaiser San Diego approach: https://twitter.com/MatthewBowdish/status/1087910300773273600
Cross-Reactions between PCN and Cephalosporins mainly related to side-chain similarity JACI-IP 2018;6:1662 - Avoid aminocephalosporins in PCN allergic pts?
https://twitter.com/MatthewBowdish/status/1087912076121501696
This is a Twitter summary from the 2019 WSAAI meeting. This summary was compiled from the tweets posted by Matthew Bowdish @MatthewBowdish and Ray Firszt @RayFirszt, who attended the 2019 Western Society of Allergy, Asthma and Immunology (WSAAI) meeting. The tweets were labeled #WSAAI. The text was edited by me.
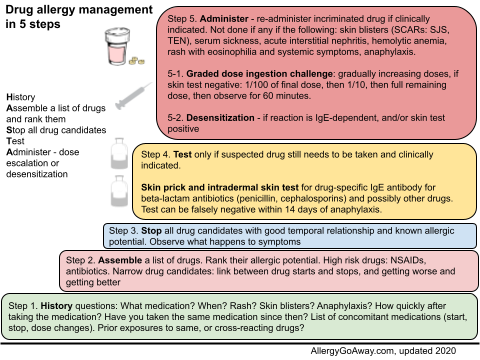
Drug allergy management in 5 steps (click to enlarge the image).
92% of patients with difficult to control asthma had at least one medical comorbidity. What were those comorbidities? Obesity, anxiety/depression, GERD, cardiovascular disease. Asthma: 90% of pts with severe asthma have at least one comorbidity, 70% have more than 2. Many co-morbidities are bi-directional, ie if you treat one, you get improvement in the other and vice versa.
Non pharma management of asthma: exercise - high intensity, diet - high protein/low glycemic diet - you need both to improve asthma control.
Step down RX for asthma who are well controlled for 3 months: stopping LABA was associated with greater decline in lung function and more hospitalizations, maybe we need longer than 3 months of control.
Pts who cough and failed ICS/LABA combo inhaler improved with Spiriva. Likely through modulating cough reflex sensitivity, despite no difference in FEV1.
Only 22% of large group of health care providers used asthma inhalers correctly (JACI-IP 2018;6:987). Most common specific errors of healthcare professionals with not using their inhalers correctly: https://twitter.com/MatthewBowdish/status/1087905408486825984
Check our JACI-IP 2018;6:1246 for interesting article on skin testing for suspected iodinated contrast media hypersensitivity.
For contrast reactions: consider SPT :prick undiluted, ID 1:10 dilution - not irritating. Pretreatment for contrast reactions does not appear to be helpful. Approach to RCM reactions: https://twitter.com/RayFirszt/status/1087908037426204674
Controversies in beta-lactam allergy covered in JACI-IP:
1. Role of skin testing vs direct challenge
2. Length of challenge (single dose vs multiple day)
3. Cephalosporin cross-reactivity with PCN and other cephalosporins
Optimal length of penicillin challenge is unclear. 5 days seems reasonable to rule out delayed non severe reactions.
Current Kaiser San Diego approach: https://twitter.com/MatthewBowdish/status/1087910300773273600
Cross-Reactions between PCN and Cephalosporins mainly related to side-chain similarity JACI-IP 2018;6:1662 - Avoid aminocephalosporins in PCN allergic pts?
https://twitter.com/MatthewBowdish/status/1087912076121501696
This is a Twitter summary from the 2019 WSAAI meeting. This summary was compiled from the tweets posted by Matthew Bowdish @MatthewBowdish and Ray Firszt @RayFirszt, who attended the 2019 Western Society of Allergy, Asthma and Immunology (WSAAI) meeting. The tweets were labeled #WSAAI. The text was edited by me.
Drug allergy management in 5 steps (click to enlarge the image).