This is a Twitter summary from the 2019 WSAAI meeting. This summary was compiled from the tweets posted by Matthew Bowdish @MatthewBowdish and Ray Firszt @RayFirszt, who attended the 2019 Western Society of Allergy, Asthma and Immunology (WSAAI) meeting. The tweets were labeled #WSAAI. The text was edited and modified by me.
Dr. Woessner presented on drug allergy.
Adverse drug reaction classification: https://twitter.com/RayFirszt/status/1088157697013235712
Drug hypersensitivity is an immune mediated reaction to a pharmaceutical agent or its excipients.
Delayed reactions
Fluoroquinolones cause delayed maculopapular eruptions in 2% of pts. These reactions are self limiting and T-cell mediated. Patch testing is not useful. The reaction does not seem to be reproducible as many patients getting oral challenge did not react again. There is 50% cross reactivity between different fluoroquinolones.
Management of fluoroquinolone delayed reactions: https://twitter.com/RayFirszt/status/1088159523536199680
Immediate reactions
Immediate reactions to fluoroquinolones occur within 1 hr, there is 50% cross reactivity. Many patients will tolerate on reexposure. Non irritating concentrations for SPT/ID testing for fluoroquinolones: https://twitter.com/RayFirszt/status/1088160135870959618
What to do with skin results: https://twitter.com/RayFirszt/status/1088160626717843456
Macrolides rarely cause IgE-mediated reactions. Most likely presentation is maculopapular reaction. You can skin test with azithromycin 0.01 mg/ml.
Antibiotics that rarely cause immune reactions: https://twitter.com/RayFirszt/status/1088164023588159488
Performing drug challenges: https://twitter.com/RayFirszt/status/1088165276921655297
If delayed reactions, consider doing drug challenges over several days. You can do placebo challenges by buying capsules and filling them with flour or other substance. Obtain consent for challenges, and specifically, for use of placebo.
Multiple drug allergy syndrome: history of adverse drug reactions to 2 or more medications that appear to be immune mediated. History tips: https://twitter.com/RayFirszt/status/1088161822539010048
Multiple drug intolerance syndrome: more than 3 different classes of drugs with no evidence of immune reactions. Usually side effects. Difficult to treat. Consider placebo challenges. Sometimes need psychology involvement if they’re having conditioned responses.
Gell-Coombs type II mediated immune reactions: https://twitter.com/RayFirszt/status/1088162661672542208
Type IV: https://twitter.com/RayFirszt/status/1088163014858010624
“Baboon syndrome” is systemic contact dermatitis secondary to topical sensitization. Sharply demarcated rash, involves flexural or intertriginous area.
Sulfa sensitivities: usually skin reactions. They can be IgE-mediated or severe delayed reactions. There is no validated skin test. Avoid sulfa antibiotics unless critical. Non-antibiotic sulfonamides are safe, like diuretics or Diamox.
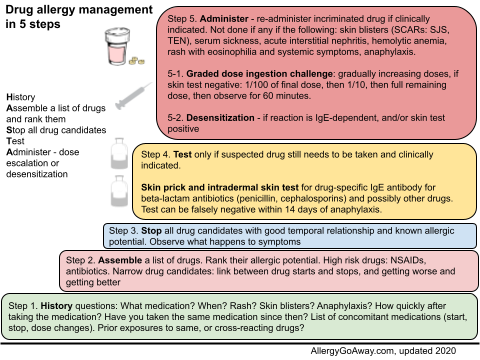
Drug allergy management in 5 steps (click to enlarge the image).
Dr. Woessner presented on drug allergy.
Adverse drug reaction classification: https://twitter.com/RayFirszt/status/1088157697013235712
Drug hypersensitivity is an immune mediated reaction to a pharmaceutical agent or its excipients.
Delayed reactions
Fluoroquinolones cause delayed maculopapular eruptions in 2% of pts. These reactions are self limiting and T-cell mediated. Patch testing is not useful. The reaction does not seem to be reproducible as many patients getting oral challenge did not react again. There is 50% cross reactivity between different fluoroquinolones.
Management of fluoroquinolone delayed reactions: https://twitter.com/RayFirszt/status/1088159523536199680
Immediate reactions
Immediate reactions to fluoroquinolones occur within 1 hr, there is 50% cross reactivity. Many patients will tolerate on reexposure. Non irritating concentrations for SPT/ID testing for fluoroquinolones: https://twitter.com/RayFirszt/status/1088160135870959618
What to do with skin results: https://twitter.com/RayFirszt/status/1088160626717843456
Macrolides rarely cause IgE-mediated reactions. Most likely presentation is maculopapular reaction. You can skin test with azithromycin 0.01 mg/ml.
Antibiotics that rarely cause immune reactions: https://twitter.com/RayFirszt/status/1088164023588159488
Performing drug challenges: https://twitter.com/RayFirszt/status/1088165276921655297
If delayed reactions, consider doing drug challenges over several days. You can do placebo challenges by buying capsules and filling them with flour or other substance. Obtain consent for challenges, and specifically, for use of placebo.
Multiple drug allergy syndrome: history of adverse drug reactions to 2 or more medications that appear to be immune mediated. History tips: https://twitter.com/RayFirszt/status/1088161822539010048
Multiple drug intolerance syndrome: more than 3 different classes of drugs with no evidence of immune reactions. Usually side effects. Difficult to treat. Consider placebo challenges. Sometimes need psychology involvement if they’re having conditioned responses.
Gell-Coombs type II mediated immune reactions: https://twitter.com/RayFirszt/status/1088162661672542208
Type IV: https://twitter.com/RayFirszt/status/1088163014858010624
“Baboon syndrome” is systemic contact dermatitis secondary to topical sensitization. Sharply demarcated rash, involves flexural or intertriginous area.
Sulfa sensitivities: usually skin reactions. They can be IgE-mediated or severe delayed reactions. There is no validated skin test. Avoid sulfa antibiotics unless critical. Non-antibiotic sulfonamides are safe, like diuretics or Diamox.
Drug allergy management in 5 steps (click to enlarge the image).