Wheeze patterns in young children vary over time and with treatment, rendering the distinction between episodic viral wheeze and multiple-trigger wheeze unclear in many patients.
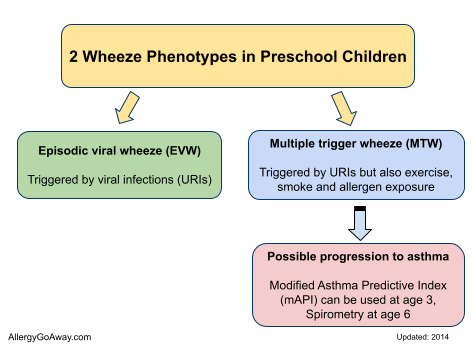
Preschool wheeze can be divided into:
- “episodic viral” wheeze (EVW) - triggered by URIs
- “multiple trigger” wheeze (MTW) - triggered by URIs but also exercise, smoke and allergen exposure
These 2 phenotypes can change within an individual over time.
Wheeze Phenotypes in Preschool Children (click to enlarge the image):
Inhaled corticosteroids remain first-line treatment for multiple-trigger wheeze, but may also be considered in patients with episodic viral wheeze with frequent or severe episodes, or when the clinician suspects that interval symptoms are being under reported.
Any controller therapy should be viewed as a treatment trial, with scheduled close follow-up to monitor treatment effect.
Oral corticosteroids are not indicated in mild-to-moderate acute wheeze episodes and should be reserved for severe exacerbations in hospitalized patients. Future research should focus on better clinical and genetic markers, as well as biomarkers, of disease severity.

Modified Asthma Predictive Index (mAPI) (click to enlarge the image). A positive mAPI greatly increased future asthma probability (eg, 30% pretest probability to 90% posttest probability) http://buff.ly/ZJfMgQ
References:
Classification and pharmacological treatment of preschool wheezing: changes since 2008. Paul L.P. Brand et al. ERJ April 1, 2014 vol. 43 no. 4 1172-1177.
http://erj.ersjournals.com/content/43/4/1172.short
Preschool wheeze can be divided into:
- “episodic viral” wheeze (EVW) - triggered by URIs
- “multiple trigger” wheeze (MTW) - triggered by URIs but also exercise, smoke and allergen exposure
These 2 phenotypes can change within an individual over time.
Wheeze Phenotypes in Preschool Children (click to enlarge the image):
Inhaled corticosteroids remain first-line treatment for multiple-trigger wheeze, but may also be considered in patients with episodic viral wheeze with frequent or severe episodes, or when the clinician suspects that interval symptoms are being under reported.
Any controller therapy should be viewed as a treatment trial, with scheduled close follow-up to monitor treatment effect.
Oral corticosteroids are not indicated in mild-to-moderate acute wheeze episodes and should be reserved for severe exacerbations in hospitalized patients. Future research should focus on better clinical and genetic markers, as well as biomarkers, of disease severity.
Modified Asthma Predictive Index (mAPI) (click to enlarge the image). A positive mAPI greatly increased future asthma probability (eg, 30% pretest probability to 90% posttest probability) http://buff.ly/ZJfMgQ
References:
Classification and pharmacological treatment of preschool wheezing: changes since 2008. Paul L.P. Brand et al. ERJ April 1, 2014 vol. 43 no. 4 1172-1177.
http://erj.ersjournals.com/content/43/4/1172.short